Position Paper of the World Organization of Dermophthalmology (WOD)
Abstract
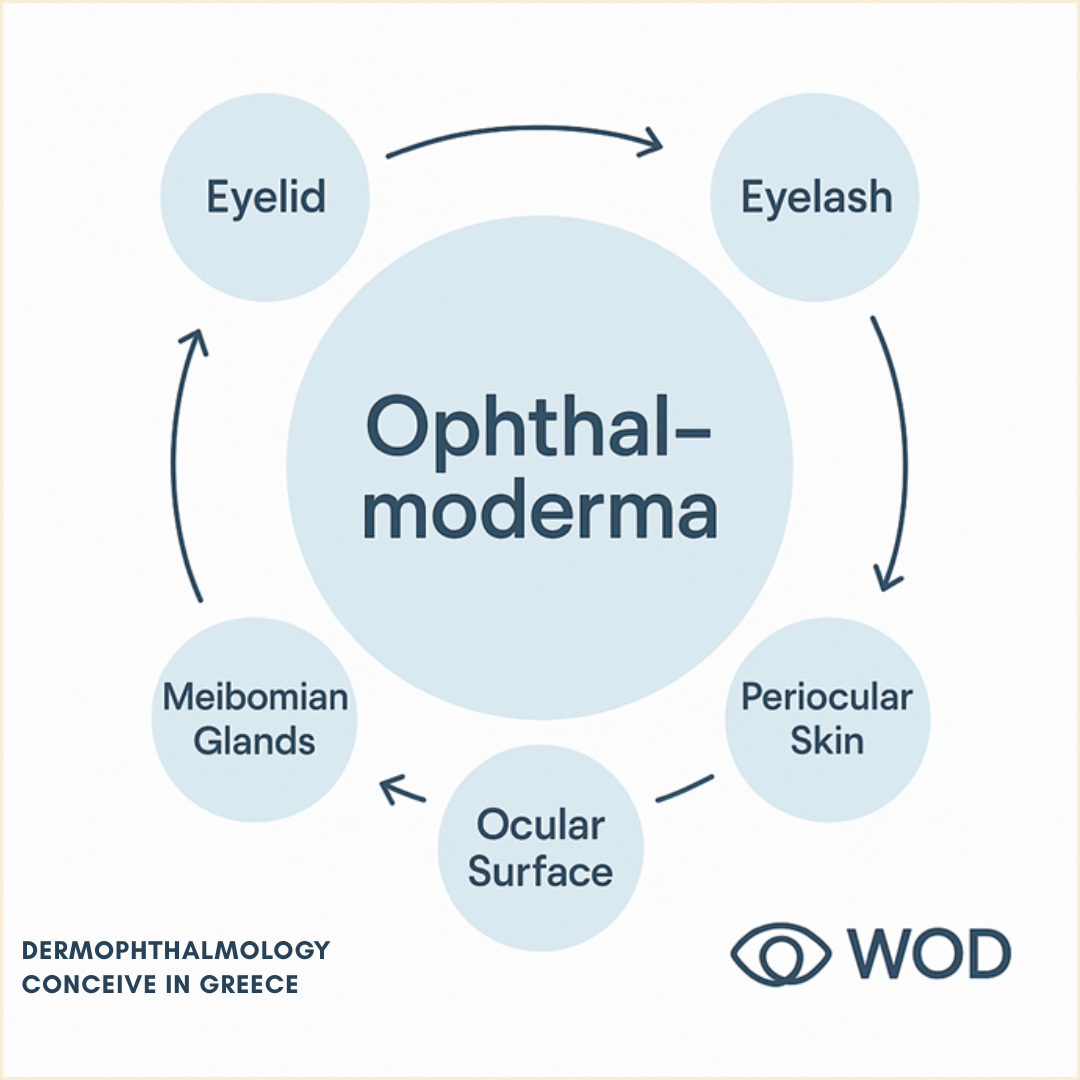
Classical Anatomy and Physiology have traditionally treated organs as separate structures with clear boundaries: eye, skin, hair, mucosa.The zones where these systems meet – the interfaces – were viewed merely as “transitional areas” between organs, not as autonomous biological systems.Dermophthalmology introduces the concept of Ophthalmoderma as a single target organ that includes:
- the eyelids,
- the eyelashes,
- the Meibomian and associated glands,
- the ocular surface, and
- the periocular skin.
Ophthalmoderma is defined as an interface organ in which skin, hair and ocular surface function as one continuous system, regulating:
- lubrication,
- thermo–hygrometric balance,
- microbial ecology, and
- ultimately the quality of vision and the aesthetic expression of the gaze.
This Position Paper:
- presents Ophthalmoderma as a new biological and clinical model,
- establishes the concept of dual interfaces (Meibomian–Follicle Axis, Tear–Skin Axis, Ophthalmo–Dermal Interface),
- introduces a structural and functional analogy with the Periodontium and Periodontology,
- proposes a new definition of eye health:
Eye health is not a property of a single organ,
but a harmony of interfaces – between skin, tear and vision.
Key Points
- Ophthalmoderma is recognized as a new target organ uniting skin, lashes, eyelids and ocular surface into a single functional system.
- Dermophthalmology introduces the model of dual interfaces:
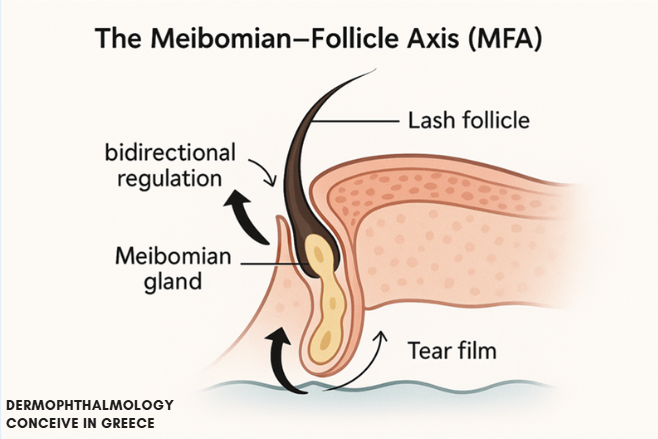
- Meibomian–Follicle Axis (MFA)
- Tear–Skin Axis (TSA)
- Ophthalmo–Dermal Interface (ODI)
- A new foundational definition of eye health is proposed:
Eye health is harmony between skin, tear and vision.
- The analogy with the Periodontium shows that Ophthalmoderma for the eye is what the Periodontium is for the tooth: the key organ of prevention.
Chapter 1. The Paradox of Ocular Anatomy
1.1 Why the Interface Was Ignored
Classical Medicine was built on a structural model:
organ = clear borders + specific tissues + distinct pathology.
Thus:
- the eye was defined as a visual organ,
- the skin as a protective cover,
- the glands as secretory units,
- the hairs as secondary appendages.
The regions where these systems meet –the eyelids, the eyelashes, the ocular surface – were considered merely:
- anatomical “boundaries”, or
- “transition areas” between organs.
This created a paradox:in the most exposed and sensitive organ of the human body – the eye –its surface, the point of contact with the external world, was never recognized as an autonomous target organ.
1.2 The Gap in Ophthalmology
For decades, Ophthalmology focused primarily on:
- the cornea,
- the crystalline lens,
- the retina,
- intraocular surgery (cataract, vitreous, glaucoma).
The eyelid, the lashes and the Meibomian glands were treated as:
- “peripheral structures”, or
- local problems (blepharitis, chalazion, MGD),
not as parts of a unified organ.
As a result:
- dry eye symptoms,
- contact lens intolerance,
- aesthetic fatigue of the gaze
have often been managed fragmentarily, without a single integrative model.Dermophthalmology is introduced precisely to fill this conceptual and clinical gap.
Chapter 2. From Interface to Organ – The Ophthalmoderma Concept
2.1 The Foundational Idea
Ophthalmoderma is defined as:the unified interface organ in which skin, eyelashes, glands, tear film and ocular surface function as one continuous biological system.
It includes:
- Eyelid skin (epidermis, dermis, subcutaneous tissue)
- Eyelash follicles and lashes
- Glands: Meibomian, Zeis, Moll
- Ocular surface: conjunctiva, cornea, tear film
- Periocular skin and eyebrows as functional regulators.
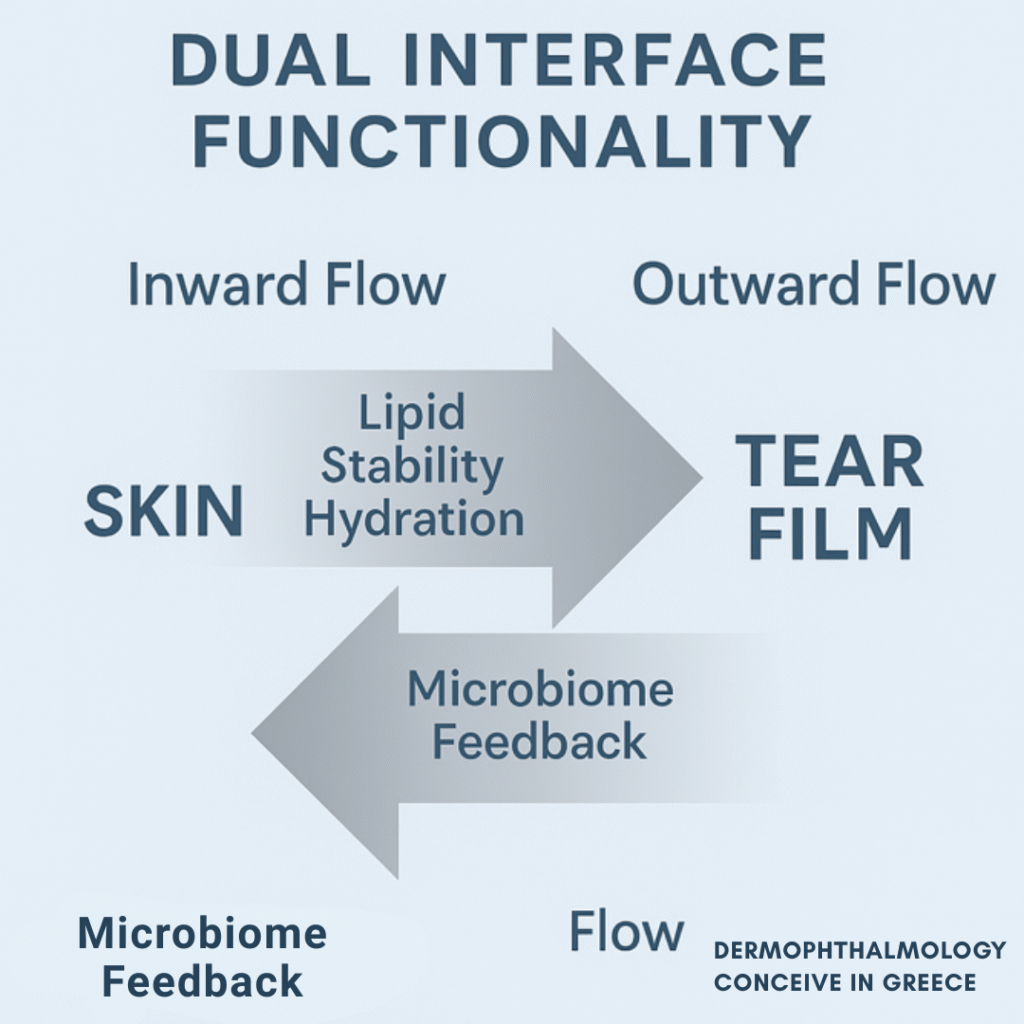
2.2 Dual Interface Functionality
Ophthalmoderma is not a static boundary.It is a field of bidirectional flow:Inward flow – from skin, glands and lashes → towards the tear film and ocular surface
- lipid stabilization,
- reduction of evaporation,
- protection of the cornea,
- optical clarity.
Outward flow – from tear film & ocular surface → towards the skin and lash follicle
- evaporation & humidity regulation,
- microbial transfer,
- sensory feedback (blink reflex, foreign body sensation),
- influence on skin, follicle and hair.
The function of Ophthalmoderma is symmetrical:each movement is simultaneously:
- protection of the eye, and
- regulation of skin and hair.
Chapter 3. The “Law of Interfaces” in Biology
In every living system there is an active interface –the place where two environments meet and exchange:
- energy,
- matter,
- information
Examples:
|
System |
Interface |
Dual Function |
|
Brain |
Blood–Brain Barrier |
Protects brain ↔ regulates transfer of substances & signals |
|
Lungs |
Air–Blood Interface |
Gas exchange (O₂/CO₂) ↔ regulation of surface tension & immunity |
|
Heart |
Endocardium–Blood |
Conducts electrical signals ↔ responds to mechanical load |
|
Skin |
Skin–Microbiome Interface |
Physical barrier ↔ immune & neuro-sensory communication |
|
Eye |
MFA &Ophthalmoderma |
Lipid outflow to tear film ↔ feedback from follicle, microbiome & environment |
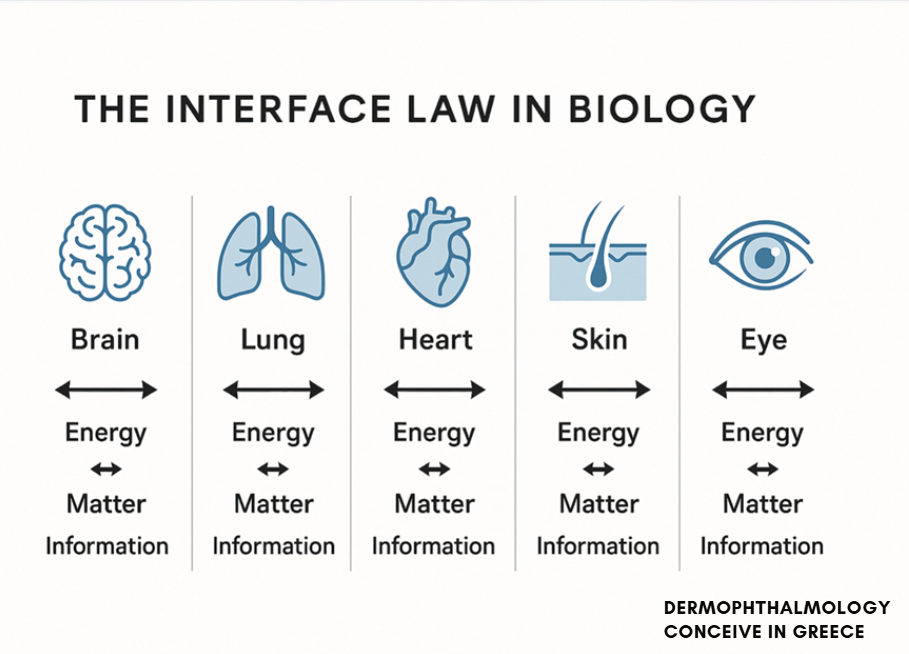
Until now, Medicine has treated these areas as “organ borders”,not as organs in their own right.With the concept of Ophthalmoderma, Dermophthalmology does something fundamentally new:It elevates the interface (eyelid–eyelash–ocular surface) to a target organwith its own biology, pathology and therapeutics.
This constitutes a true paradigm shift in the sense of Thomas Kuhn:a new theoretical framework that explains phenomena the previous model could not integrate.
Chapter 4. The Biological Foundation of Ophthalmoderma
4.1 Embryologic Unity – The Ectoderm
All elements of Ophthalmoderma:
- eyelid skin,
- Meibomian / Zeis / Moll glands,
- eyelash follicles,
- ocular surface
originate from the ectoderm.
Niyazov D. et al., Dev Biol, 2018
Cotsarelis G., J Invest Dermatol, 2006
This means they are:
- histologically related,
- functionally continuous,
- pathophysiologically interconnected.
Therefore:
- skin diseases (rosacea, seborrheic dermatitis, psoriasis) can affect Meibomian glands and the ocular surface;
- ocular surface inflammation and MGD can have cutaneous and trichologic manifestations.
The eye does not “end” at the lid margin –it continues through it.
4.2 The Microbiome of Ophthalmoderma
The microbiome of the eyelids and ocular surface forms a single ecosystem, including:
- Staphylococcus, Corynebacterium, Cutibacterium,
- Demodexfolliculorum / brevis,
- and other commensal organisms.
Zegans M. & Van Gelder R., CurrOpinMicrobiol, 2020
Peral A. et al., Ocul Surf, 2023 – “The ocular–skin microbiome continuum.”
Dermophthalmology:
- does not view blepharitis as a “local infection”
- but as interface dysbiosis – loss of ecological balance.
Therapeutic goal:
not sterilization,
but restoration of a balanced biofilm
through gentle cleansers, thermal regulation, and targeted actives (e.g. tea tree oil).
4.3 Lipid Continuity – From Gland to Tear Film
The Meibomian glands, under the influence of skin, hormones and local environment, produce meibum which:
- forms the lipid layer of the tear film,
- reduces evaporation,
- stabilizes the optical surface.
Baudouin C. et al., Prog Retin Eye Res, 2016
McDonald M. et al., Eye Contact Lens, 2014
Dysfunction leads to:
- Meibomian Gland Dysfunction (MGD),
- evaporative dry eye,
- surface inflammation,
- madarosis (lash loss) via follicular inflammation.
Dermophthalmology views this not as three separate diseases,but as one Ophthalmoderma dysregulation syndrome.
Chapter 4A. Components of Ophthalmoderma& Their Functions
- a) Eyelid Skin
- The thinnest skin of the body.
- Contains sebaceous and sweat glands.
- Regulates:
- temperature,
- humidity,
- pH,
- exposure to external factors (make-up, pollution).
Dysfunction → erythema, dermatitis, rosacea → fosters MGD & blepharitis.
- b) Follicle & Eyelash – Air-Tunnelling& Hydration
The eyelash is:
- a sensory hair (triggers blink reflex),
- a mechanical shield,
- an aerodynamic regulator of tear evaporation.
Hu D. & Mitchell G., J R Soc Interface, 2015
Air-tunneling effect:
- optimal lash length and density create a calm airflow zone in front of the cornea,
- reduce air velocity at the surface,
- protect against evaporation (up to ~50%),
- preserve hydration of the ocular surface.
The follicle:
- hosts Demodex, bacteria and Zeis/Moll glands,
- is a micro-ecosystem where hair, lipids, microbes and immunity intersect.
Dysregulation (dysbiosis, MGD, cosmetic overload) →
- folliculitis,
- madarosis,
- altered lash curvature/length,
→ accelerated evaporation & dry eye.
- c) Meibomian Glands
- The central “lipid factory” of Ophthalmoderma.
- Function as a two-way pump:
- towards the tear film (lipids, tear film stability),
- towards the lash/skin (follicle nourishment, hair shine, local immunity).
Dysfunction → MGD →dryness, burning, redness and aesthetic fatigue of the gaze.
- d) Ocular Surface & Tear Film
- The level where light meets biology.
- Composed of:
- corneal and conjunctival epithelium,
- aqueous phase of the tear,
- mucin and lipid layers.
Tear film stability:
- depends on the coordinated function of glands, skin and eyelashes,
- determines the quality of vision, comfort and blink dynamics.
- e) Eyebrows & Periocular Skin
- Divert sweat and fluids away from the eye.
- Contribute to emotional expression and the visual framing of the gaze.
- Function as a superior protective “arch”.
Their omission in diagnosis leaves room for hidden foci of inflammation (seborrheic, psoriatic involvement).
Chapter 4B. The Periodontal Analogy
- Before the Birth of the Periodontium Concept
Before the 20th century, Dentistry:
- focused on the tooth,
- considered gingivitis and bone loss “local complications”.
There was no real concept of the Periodontium –the ecosystem that:
- supports,
- nourishes,
- protects the tooth.
- Emergence of the Periodontium as an Organ (1900–1930)
Researchers such as Gottlieb, Orban and Glickman defined the Periodontium as:
- gingiva,
- alveolar bone,
- periodontal ligament,
- root cementum.
Dentistry moved:from “treating the tooth”to “caring for the system that supports it”.
- The Periodontal Revolution
From the 1950s onwards:
- Periodontology became an autonomous specialty.
- Oral hygiene became a daily preventive habit (tooth brushing, flossing, professional cleanings).
- Disease began to be understood as biofilm dysbiosis, not simply “infection”.
- Ophthalmoderma as the Ocular Equivalent
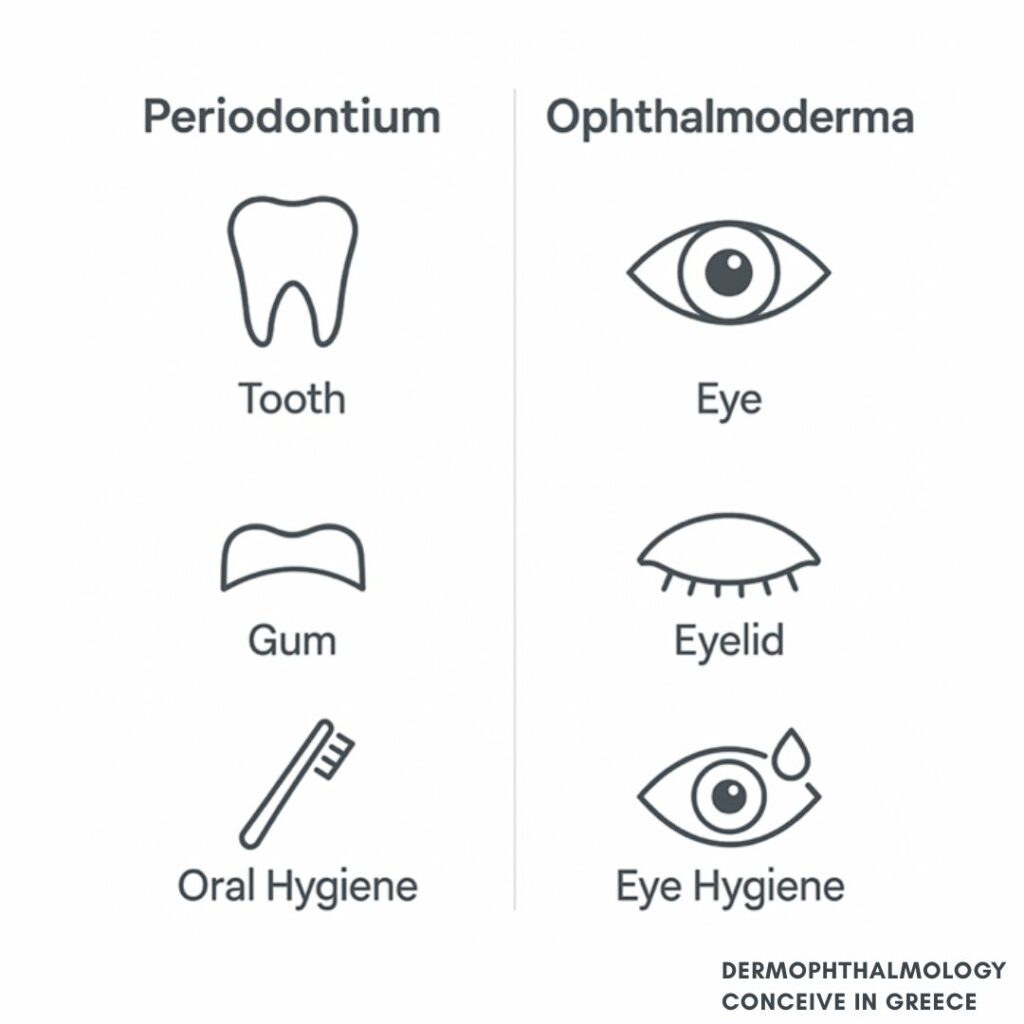
What the Periodontium is to the tooth,Ophthalmoderma is to the eye:
Periodontium | Ophthalmoderma |
Tooth | Eye |
Gingiva, ligament, bone | Eyelid, eyelashes, glands, ocular surface |
Periodontium | Ophthalmoderma |
Plaque / biofilm | Demodex / lipid imbalance / lid biofilm |
Daily tooth brushing | Daily eyelid hygiene |
“Oral Hygiene” | “Eye Hygiene” |
Protection of teeth | Protection of vision |
In both systems:inflammation starts at a dirty interface that is not cleaned regularly,and progresses to destruction of the supporting apparatus.
- Comparative Biological Analysis
Parameter | Periodontium | Ophthalmoderma |
Location | Interface bone–mucosa/tooth | Interface skin–ocular surface |
Tissues | Bone, cementum, gingiva, ligament | Skin, follicle, glands, tear film, conjunctiva |
Function | Support & protection of the tooth | Lubrication & protection of the eye |
Microbiome | Dental plaque / oral biofilm | Lid/ocular biofilm |
Pathology | Gingivitis, periodontitis | Blepharitis, dry eye |
Health key | Daily oral hygiene | Daily ocular/eyelid hygiene |
- Preventive Analogy
“As we brush our teeth, we must also ‘brush’ our eyes.”
- Periodontium → daily brushing & flossing.
- Ophthalmoderma → daily eyelid cleansing, warm masks, gentle sprays.
Dermophthalmology brings to Ophthalmology what Periodontology brought to Dentistry:a shift from treatment to conscious daily prevention.
Chapter 5. Significance of This Article
This WOD Position Paper is a foundational document for the birth of Dermophthalmology and Ophthalmoderma as a new target organ.
Its significance appears on four levels:
5.1 Scientific – Medical Value
- Introduces, for the first time internationally, the term Ophthalmoderma as a new target organ.
- Unifies scattered findings from:
- ocular surface,
- MGD,
- blepharitis,
- dermatologic/trichologic disorders
into a single coherent framework.
- Establishes dual interfaces (MFA, TSA, ODI) as biological axes.
5.2 Impact on Ophthalmology
- After Ocular Surface Disease (TFOS DEWS II), Ophthalmoderma is the next major conceptual step:
- it shifts the focus from symptom → to surface,
- and from surface → to interface.
- Provides a conceptual basis for what clinicians feel but lacked a name for:
- why MGD, blepharitis, dry eye, make-up, contact lenses and rosacea “cluster” in the same eye.
5.3 Impact on Medical Philosophy
- Moves Medicine:
- from isolated structures,
- to the harmony of interfaces.
- Aligns with major paradigm shifts:
- cellular pathology (Virchow),
- microbiome & ecological health,
- neuroendocrinology,
and adds Interface Medicine as a new level of understanding.
5.4 Communicational & Social Impact
- Creates a clear preventive message for the public:
“Just as Dentistry established oral hygiene,
Dermophthalmology establishes ocular hygiene.”
- Opens the way for:
- new Eye Hygiene protocols,
- a new product category (Ophthalmo-Cosmetics),
- a new educational culture among ophthalmologists, dermatologists and aesthetic practitioners.
Chapter 6. Conclusion & Future Directions
Ophthalmoderma:
- is not just a new term;
- it is a new way of seeing:
- the eye,
- the skin,
- and the human body as a network of interfaces.
Dermophthalmology:
- gives Ophthalmology a new field of action,
- returns to the Hippocratic principle of harmony,
- and transforms eye health from a narrow biomedical notion into:
a holistic harmony between skin, tear and vision.
This Position Paper is the official founding declaration of Ophthalmoderma:
- what the first texts on Ocular Surface once were,
this paper now is for Dermophthalmology and Ophthalmoderma.
Authorship (Authority & Contributions)
Prepared by the Scientific Team of the World Organization of Dermophthalmology (WOD) under the conceptual leadership of John Tsakalos,with reference to the works of international ophthalmologists and researchers including Marguerite McDonald, Christophe Baudouin, Stephen C. Pflugfelder, Kazuo Tsubota, Aníbal Peral, Dmitry Niyazov, George Cotsarelis, Michael Zegans, and Russell Van Gelder, whose pioneering research has contributed to the advancement of ocular surface scienceand to the conceptual foundation of Dermophthalmology and the Ophthalmoderma model.
WOD also acknowledges the contribution of David Hu and Guillermo Mitchell (2015)for their pioneering aerodynamic studies on eyelash airflow protection and the air-tunneling effect,which provide an essential physical–biological dimension to the functional understanding of Ophthalmoderma.
With gratitude to the Hellenic Ophthalmological Community,whose clinical insight and educational initiativeshave supported the dissemination of eyelid and ocular surface hygiene. (For educational and scientific purposes – Athens, 2025)
Citation Format
World Organization of Dermophthalmology (WOD).
Ophthalmoderma– The New Target Organ in Dermophthalmology.
WOD Position Paper, Athens, Greece, 2025.
Edited by John Tsakalos.
Scientific Motto
“Where Eye Health meets Skin Science.”
Where the health of the eye meets the science of the skin.
